
Understanding W-Sitting: Risks, Causes, and How to Help Your Child
Let’s begin with, understanding what W-sitting is? W-sitting is when children sit with their knees bent, feet tucked in under their bottom and resting on the floor between their legs and with their legs out to the sides.

The child’s knees and thighs may be touching together or spread apart. It is usually noticeable in children from the ages between 3-6 years old but sometimes it can show in both younger and older children. W-sitting can be a potentially harmful position in which to sit. This position adjusts the knee and the hip joints by positioning them in this way which they are not anatomically designed to support. If you think of your own knees, knees are like hinges. They are designed for this, but they are not designed to move in rotational patterns, which W-sitting does.
Why do children W-sit? Children may develop a habit of sitting this way. This can be a way of giving them more stability in their little bodies when they have difficulty with the crisscross position. You would usually see this when children are on the floor or seated in a group. Maybe playing with blocks or puzzles. Children who have low core strength may prefer to use the W-sitting position to gain more stability in their positioning and even to help them use both hands in an activity.
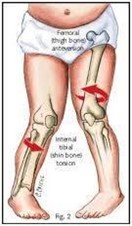
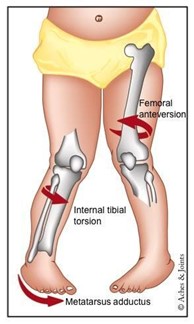
Overtime undeveloped bones and joints are affected by routine stress. Internal rotation of the thigh bone is called the ‘femoral anteversion.’ Is typical at a young age and seems to decrease after age 8, but therapists see better results the earlier the problem is looked at to correct it as early as possible. Sometimes it can also be seen in children with underlying issues, such as low tone, muscle weakness, sensory concerns and decreased fine and gross motor coordination.
In the w-pose children do not have to work as hard to engage their core and hold their core upright. Instead, they spread their lower limbs to create a wider base of support, relying on their joint structures instead of their muscles to hold them up. This increased posterior pelvic tilt, which is when the front of the pelvis rises, and the back of the pelvis drops. This can result in poor sitting posture, low core activation and delayed fine motor development. This wide base also limits a child’s need to weight shift on their bottom from one side to the other during play. This would result in decreased use of balance responses.
Lack of activation causes a cycle of muscle weaknesses and resulting in difficulty integrating the left and right sides of the body which then leads to decreased coordination. This can possibly lead to decreased play involving crossing over the body’s midline and poor progress with high-level fine motor tasks in using two hands.
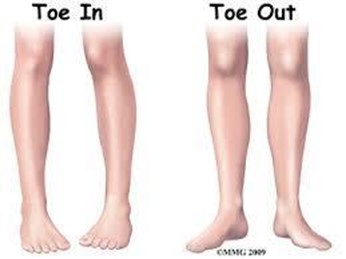
Increasing the inward rotation of the hip while decreasing outward range of motion can contribute to Pigeon-toe gait pattern. This is a walking pattern which can contribute to excessive tripping, clumsiness, instability when walking and running. Another joint abnormality that may occur is called ‘tibial torsion’, which is the outward rotation of the lower leg and while standing the foot turns outward with the knee turning inward. It can be painful and affect the way the child walks and runs.

When to seek help?
If a child………….
- Develops a limp
- Weakness in lower extremities
- Uses a pigeon- toed gait
- Low muscle tone or weak core strength
- Unable to sit alone in any one position other than ‘W’
- Clumsy or uncoordinated
- Trouble with fine motor tasks.
Alternatives:
Provide a simple cue, phrase, or word to remind the child to correct his/her leg position. Every time you see it happen you need to make the child aware of the position and that it needs to be changed. Do not make the child feel insecure. You should make it light and fun for example, ‘Sarah legs, Sarah legs, Sarah Sarah legs legs legs.’ In a song tune or rhyme. Smile while you sing it, and the child will too and even the child’s friends at school will learn it and help to encourage ‘Sarah.’ I even had a child correct Sarah’s legs when she noticed the position. It was done in a gentle calm manner that everyone was happy, and we said thank you.
Other sitting options:
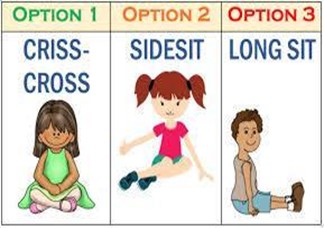
- cross-legged/crisscross, with feet crossed and knees apart
- Side-sit: knees bent, weight shifted to one hip and both feet are on the same side. This takes away stress from the hip joint structures for easy transitions in and out of sitting. Encourage sitting both right and left sides for equalization and development.
- Long-sit: feet straight in front of child
- Short kneel sit back against heels folded in kneeling position with feet tucked under bottom.
- Half-kneel: 1 foot tucked under and other foot flat on ground
- Squat- great way to stabilize core and activate the glutes and hamstrings which will increase overall strength.
- Chair sit: If struggling with other positions, sit on a low chair for a limited amount of time to encourage muscle activation.
- Lying on tummy, propped up on elbows
- Lying on back, propped up on elbows.
The stability of W-sitting lets the child play with toys in an upright sitting position without having to worry about falling over. This needs to change as quickly as possible to avoid future problems. It is common and can be normal for children to move in and out of the position when playing on the floor, but problems begin from this position when a child sits in the position for long periods at a time.
W sitting can also increase risk of hip dislocation, more likely if a child already has Dysplasia, which may not even have been diagnosed at the time. When sitting in this position you are unable to rotate the upper body, and this can make it hard for the child to reach across and perform tasks that use both hands together and by crossing their arm over from one side to another. In time this could potentially affect the way to perform writing skills and other important tabletop activities.
It is very important to keep making the correction and reminding your child in your fun way that it needs to change every time. Otherwise, it could end up impacting their growth and development in a big way. This W-sitting has been seen from a physical therapist’s perspective, which is based on years of clinical practice and observations. Children are placing their hips in a position, which is compromising the joint, which will affect the child’s young bones, which are affected by habitual patterns in which they sit.
It may aggravate the neurological issues such as low muscle tone that means when the child is not actively using their muscles those become floppier, softer, and harder to hold their little body upright. Therefore, this affects postural muscles.
It is a convenient ‘natural transition’ from crawling or kneeling to sitting. Rather do not take chances. If you have any concerns, please speak to your child’s teacher for feedback on his/her sitting at school or see an Occupational therapist to hear more about W-sitting in detail and I am sure she would be able to guide you and help with regular exercises to implement as well as assess the individual child.
References:
https://www.childsplaytherapycenter.com/w-sitting-correct/
https://lemonlimeadventures.com/when-to-worry-about-w-sitting/